
1313 words – 7 minute read
Hey! Happy Sunday. This week marks the end of my four-part series on the Obesity epidemic in the developed world.
In week one, I wrote about the scale of the crisis – over 42% of Americans are currently obese (BMI of 30 or higher); in week two, I wrote about the causes of obesity, which I identified as both biological and environmental; in week three, I wrote about the extremely apparent class divide in obesity (poorer people and people of color are both much more likely to be obese than middle-class or wealthy whites). This week, I intend to present my best solution to the obesity epidemic: incretin mimetics.
Before we get into the weeds of my preferred biopharmaceutical solution, I first want to present some environmental changes. My assessment of the crisis is that biological and environmental factors both contribute to rising rates of obesity, so it would be unwise to only address the biological factors.
The Centers for Disease control and prevention has aggregated several suggestions for policymakers at the state and local level (view all of them here). The main theme of their recommendations revolves around “implementing early care and education and family weight programs” to control obesity for the next generation. They specifically recommend education on the benefits of exercise and how to make healthy choices. Many of their solutions are wise and well informed – and I suggest you read them – but they will not be the focus of today’s newsletter.
If you, dear reader, don’t mind short tangent, another public policy solution that I found very interesting in my research for this series was the inverse relationship between obesity and public transportation use. According to one study, the extra amount of physical activity involved in using public transportation relative to use of personal vehicles actually has a significant and negative correlation with obesity rates. This means that as public transportation use goes up, obesity rates tend to go down.
This study was domestic and longitudinal – meaning it tracks public transportation use and obesity rates in selected places in the U.S. over time – but for this post, I decided to analyze international, cross-sectional data – meaning that I analyzed a snapshot of obesity rates and public transportation use in different countries in a set year. My findings are very similar to those of the researchers who conducted the aforementioned study – obesity rates and public transportation use are significantly and inversely correlated – meaning that the relationship is more than likely not due to random chance, and obesity rates tend to go down as public transportation use goes up.
This graph shows number of public transportation journeys per capita on the X-axis and obesity rate on the Y-axis. On this graph, observe the downward sloping regression line indicating an inverse relationship between obesity and public transportation use. These data were sourced from the UTIP and the World Bank. See below:
Now it’s time to go deep on my preferred solution to the biological factors of the obesity epidemic: incretin mimetics. Incretin mimetics are a class of drug that act on your body by replicating the incretin hormones that naturally secreted to control blood sugar. According to GoodRXHealth, incretin mimetics belong “to a class of medications called GLP-1 agonists. GLP-1 agonists work by mimicking a gut hormone called GLP-1 to lower blood glucose levels after you’ve eaten a meal. They also block your liver from making glucose and help you feel full for a longer period of time.”
Incretin mimetics were originally developed to treat type-two diabetes, but because of their remarkable impact on weight management, these once-niche drugs have hit the mainstream in recent years. Drugs you will likely know – like Ozempic or Trulicity – that were once reserved only for diabetics but have begun to be approved for weight loss.
I believe the expansion of incretin mimetics into weight loss applications is a wonderful thing for humanity. In my mind, ozempic and its contemporaries are the first signs of hope that future generations will be lighter, leaner, and healthier than many of us in the U.S. today.
Here, I have a graph that shows the average % of bodyweight lost on a traditional diet versus the three most popular incretin mimetics. These data are from studies conducted on Trulicity, Victoza, and Ozempic. The four interventions (traditional diet and exercise, Trulicity, Victoza, and Ozempic) are listed on the Y-axis and the corresponding % of bodyweight lost on average is shown on the X-axis. See below:
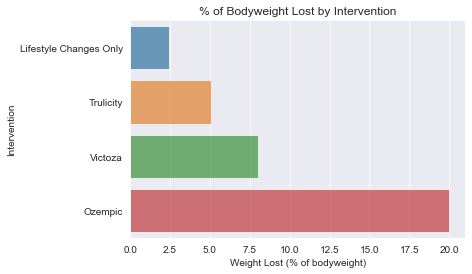
As you can very clearly see, incretin mimetics are substantially better at helping people lose weight than traditional diets – and it’s not even close.
To address the clear class disparities in obesity rates discussed in my last post, I think the federal government should subsidize the production of the incretin mimetics that have been proven to work long term. I also think Medicaid should be expanded to cover incretin mimetics in their current weight-loss formulations. Finally, patent agencies should be wary of issuing extended intellectual property protections for incremental formulation changes for incretin mimetics to prevent the virtual monopoly that has been created with insulin medication. These drugs need to be affordably available to both the rich and poor.
It might seem strange, upsetting, or unrealistic to suggest that we all jump on drugs to help us lose weight, but I would argue that it is bad public health policy to keep relying on environmental and behavioral solutions at the individual level. Studies have consistently shown that diets don’t work well long term. We need something big at the population level to address our crisis. Obesity is so strongly linked to all-cause mortality that I firmly believe pharmaceutical interventions make the most economic, political, social, and moral sense.
The biggest counterargument to this policy suggestion – and often one of the few made in good faith (looking at you, “just eat less” crowd) – is that incretin mimetics make you lighter, but not necessarily leaner. Recent studies have shown that if incretin mimetics are taken in isolation – that is, without the additions of proper diet and exercise – much of the weight lost is lean tissue. This is a very fair argument, as it is generally bad for your body to lose muscle tissue, but I think it’s missing the forest for the trees.
Many times when this argument is made – often by incredibly prominent voices in the healthcare community – it is to advocate for skipping out on drugs in favor of a traditional diet, which, in theory, results in a much better body composition when all is said and done (you lose mostly fat and often gain muscle on a well executed diet). But – and this is a big but – traditional diets just don’t work for most people. If this was the answer, we would all be skinny already. And even if most of the tissue you lose on these drugs is muscle, which I know is not ideal, your heart, lungs, joints, and tendons are all doing up to 20% less work. That will extend the number of high-quality-of-life years experienced by almost half of the population, as well as taking significant stress off of our healthcare system.
Ozempic and other drugs like it give me a lot of hope for the future, and I hope I’ve at least opened your mind to the possibility of a population-level biopharmaceutical intervention to this crisis. Also maybe we should build some more public transit. Just something to think about.
Thank you so much for joining me on this month-long journey through a topic not entirely related to the blog you subscribed to. I had so much fun diving head-first into a field of scientific research that I was interested in but that was outside of my political and economic wheelhouse. I hope you enjoyed this series as much as I did.
On a somber note, I will be stepping away from this blog for the time being to focus on my final year of undergrad. I am so excited to see what this next year holds in store for me, but school starting means I won’t have time to post here nearly as much. This goodbye is not forever, though, dear reader – you can expect sporadic posts from yours truly whenever I get a free weekend!
Thanks for reading and I’ll see you next time!

Leave a comment